Myomectomy is a surgical procedure to remove the fibroids, generally via the abdomen, without removing the womb (uterus).
What symptoms can myomectomy relieve?
Symptoms to be relieved are listed below:
- Abnormal menstrual periods leading to anaemia (>80% improvement in abnormal uterine bleeding).
- Pelvic pain.
- Back pain.
- Pressure on the bladder such as leakage, dribbling, frequent passing of urine.
- Fertility problem (infertility, premature labour, miscarriages) caused by fibroids.
- Discomfort during sexual intercourse.
How many types of myomectomy are there?
There are 2 different types of abdominal myomectomy: (a) laparoscopy (keyhole) and (b) laparotomy (open abdominal).
Key features of the two techniques are summarised below:
| Type of operation | What's involved? | Type of anaesthesia | Hospital Stay | Recovery time |
| Laparoscopy (keyhole) | Through a keyhole cut, uses a surgical instrument to remove the fibroids. | General by injection and inhalation and local. | 1 day or overnight stay. | 1 to 2 weeks |
| Laparotomy (Open) | A cut is made in the abdomen to remove the fibroids. | General: injection and inhalation. | 3 to 5 days (in some cases, 7 days) | 4 to 6 weeks |
What types of fibroids are suitable for a keyhole procedure?
Not all fibroids are suitable for laparoscopic myomectomy. Only women with one or two fibroids no larger than 7 cm in size are suitable for laparoscopic myomectomy. The location of the fibroids is also an important consideration and it is feasible to remove a pedunculated subserous fibroid larger than 7 cm in size laparoscopically.
What are the alternatives?
Not all women will have an open myomectomy as first-line treatment for fibroids; the decision is very individual following discussion with your gynaecologist. Alternatives include uterine artery embolisation or a hysterectomy.
What are the risks or complications of myomectomy?
Like all operations, myomectomy carries risks and complications. The general risks/complications applicable to both open abdominal and keyhole myomectomy are listed below:
- Excessive bleeding during the operation requiring blood transfusions.
- Anaemia due to blood loss during the operation and post-operation.
- Adverse reactions due to anaesthetics.
- Puncture of bowel or bladder during surgery.
- Opening of the womb or bowel during operation.
- If a large fibroid is removed, the wall of the womb may be weakened leaving a deep wound.
- Blood clot in legs (deep vein thrombosis) or sometimes, part of this clot can break off and travel to the lungs (known as PE). This can cause shortness of breath or even occasionally be fatal.
- Wound infection.
- Pelvic adhesion that can cause pain and/or bowel blockage, which may require surgery in the future to correct this.
- Risk of conversion to hysterectomy (although this is very low).
- A keyhole (laparoscopic) myomectomy may be converted into an open abdominal procedure for effectiveness and safety reasons.
- Eventual re-growth of fibroids. Re-treatment rates for over 5-10 years are 10% for single myomectomy and 25% for multiple myomectomy. For laparoscopic (keyhole) myomectomy, symptoms can recur in up to 2 in 5 cases within 5 years.
- Special precautions in pregnancy: consideration for the need for caesarean section delivery.
- Possible heart attack due to strain on the heart.
- Death due to severe complications during or after the operation.
What are the specific risks for keyhole myomectomy?
In addition to the above risks and complications, keyhole procedure carries its own specific risks which are listed below:
- Damage to my bowel, bladder and blood vessels may occur due to the laparoscopic technique itself. If this happens, you will need open abdominal surgery to correct the damage. Very rarely, if this damage is not recognised at the time of surgery, later surgery will be necessary.
- A keyhole (laparoscopic) myomectomy may be converted into an open abdominal procedure for effectiveness and safety reasons.
- Afterwards you may feel nauseated, feel some shoulder-tip pain and/or abdominal bloating or pain.
- You may have mild menstrual cramps and there may be some vaginal bleeding for a few days.
What sort of questions should I be asking or considering before my operation?
Points you may want to discuss when meeting your surgeon before your operation include:
- The possibility that he/she finds signs of malignant cancer in the womb during the operation. Think what action you would like him/her to do.
Would you give consent to remove the womb - Would it be beneficial for you to receive hormone treatment such as GnRH agonist for 2 to 4 months before your surgery. This may shrink the fibroids and makes removal of fibroids easier and can minimise blood loss during the operation.
- Should you consider banking your own blood before surgery in case you need it for religion or some other reasons that prevent you from receiving donor blood from the blood bank.
- As for assuring yourself that you are in good hands, you may want to ask, for examples, how many operations he/she has performed, had any of them being converted into hysterectomy.
- If you are on warfarin or blood thinning agents (e.g. Aspirin 75 mg), ask whether you should stop it and if so when.
What treatment do I get BEFORE the operation?
Depending on the size of your fibroids, it is usual to give a course of 2-3 special injections of GnRHa (1 per month) before your operation. This injection is given into your abdomen and affects the hormones in your body, putting you into a temporary menopausal state. Side effects of this medication will be explained to you when you start treatment. The injection helps shrink the fibroids, reducing the risk of excessive bleeding during the operation.
Some gynaecologists do not use GnRha
What are the risks of anaesthesia?
The risk of anaesthetic depends very much on your general health. A fit, healthy 20 year old person would be at far less risk than an 80 year old person would with some serious disease.
Possible risks of general anaesthesia are listed below:
| Nausea and Vomiting | Not always occur. May also be caused by the surgical procedure or pain relief medication. Medications and fluids may be required. This may be from a tube in the mouth or throat during anaesthetic. Cough lozenges, gargle, simple pain killer may help. |
| Muscle weakness | Muscle pain may be from spasm around the wound or the use of certain anaesthetics. Pain killers and rest usually settle it. |
| Blurred or Double vision | Usually settles down with rest. |
| Post operative pain | This is due to cuts in your skin and tissues. Resolve with painkillers and anti-inflammatory. |
| Allergic reactions | Your anaesthetist will avoid any known drugs that you know you are allergic to. In case of unexpected reaction, the team is well trained and qualified to deal with it. |
| Damage to teeth | Once you are deeply asleep, tubes may be placed inside your mouth and throat. The shape of your mouth varies and different types of dental diseases, loose teeth, bridge and crowns may be present. The anaesthetist talks about the possible damage to you before the operation. If damage occurs, you will be told about it afterwards and repair is arranged. |
What happens at pre-assessment?
At pre-assessment, certain tests are carried out to make sure that you are fit for the operation.
Possible things may be carried out by the hospital (pre-op)include:
- Pregnancy test.
- Check what medications you are taking regularly.
- Check your blood levels to see if you are fit enough to go through.
- Check blood pressure, heart rate and ECG to see if the heart is fit.
What happens ON THE DAY and BEFORE the operation?
- You will be taken to a waiting room where a nurse will check you in.
- Your surgeon may request you have an enema and a portion of your pubic hair shaved before the operation.
- An anaesthetist will meet you to go though the type of anaesthesia applicable for your case with you and ask questions on previous operation(s) if you had any and your family's.
Also, he/she will give you warnings on possible side-effects (see Table 4.) and a chance to ask questions.
Don't forget to mention any previous operation(s) you had and any side-effects. If you never had an operation under general anaesthesia, tell him/her about your family's operation(s). - In the pre-op room, an intravenous line is inserted for drugs to be given.
- You will be moved to the operating theatre where various monitors will be connected to help to care for you while you are anaesthetised.
- The anaesthetist will put you to sleep. Tube may be put into your mouth to help you to breathe and taken out at the end of the operation.
- The anaesthetist will stay with you throughout to make sure that you remain safe.
What happens DURING the operation?
What the surgeon does during the operation depend on the type of myomectomy, whether it is an open abdominal or laparoscopic (keyhole) surgery.
A. Laparoscopic (keyhole) surgery
Generally speaking, the surgeon performs the following:
- 1. Insert a catheter into the womb (uterus). Carbon dioxide gas is pumped in to inflate the abdomen to create the space for him/her to work.
- 2. Inject a blue dye to stain the womb cavity which makes it easier to locate the fibroids.
- 3. Make a small incision (cut) in the navel.
- 4. Insert the laparoscope (a specialised endoscope with fibre optic tube attached to a viewing device) into the womb to examine the abdomen.
- 5. Make two or 3 additional incisions in the abdomen. He/she will insert a special laparoscope through these incisions to find each fibroid and remove it surgically.
In some hospitals, the process is robotic assisted.
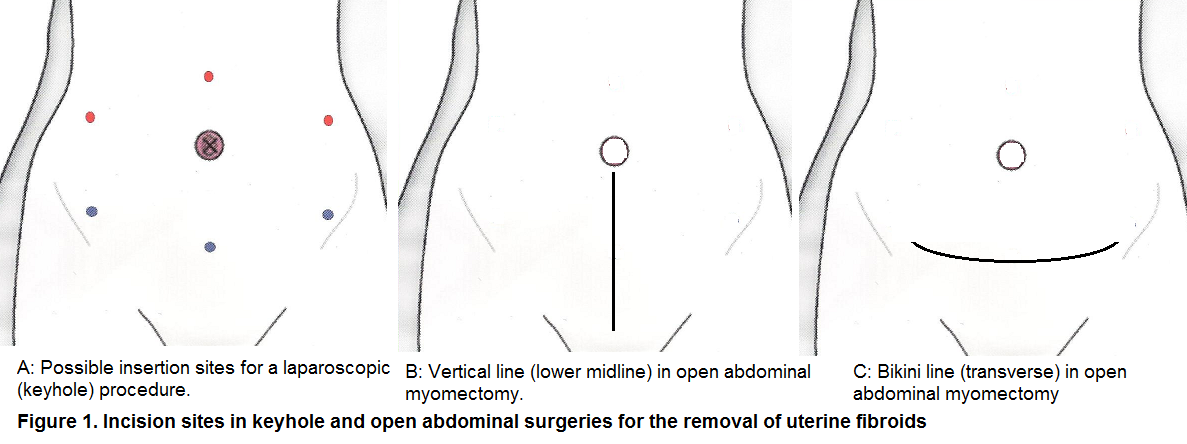
Figure 1(A) shows possible insertion sites. Your surgeon will choose them according to the size of uterus and in terms of optical viewing plus type of induction technique of the pneumoperitoneum.
- 6. After removing the fibroids, they are cut into pieces by special instruments and removed, and if necessary, the wall of the womb is repaired.
- 7. When the removal of fibroids is completed, as much gas as possible is removed.
- 8. Close up all incisions with either stitches or clamps/staples at the end of the operation.
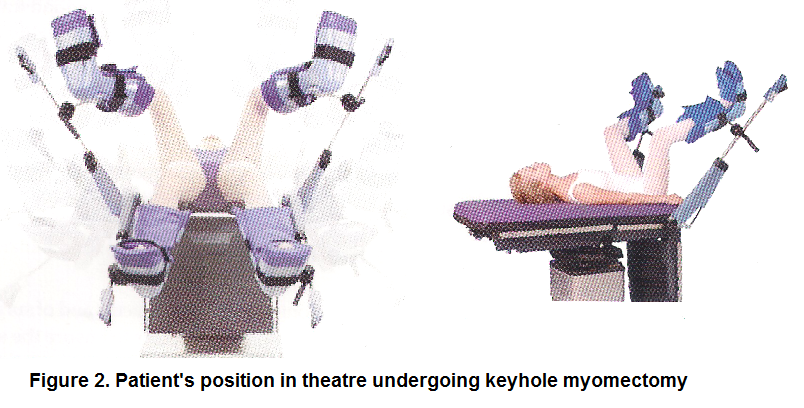
Figure 2 below shows your position in the operating theatre under keyhole procedure.
B. Open abdominal surgery
Your surgeon performs the following:
- 1. Insert a catheter into the womb (uterus) through which he/she inject a blue dye to stain the womb cavity which makes it easier to locate the fibroids.
- 2. An opening is made in the abdomen. In some cases, more than one incision is required. Generally, your scar will look like vertical line (1B) or a hair line bikini (1C) or as shown in Figure 1 above.
- 3. Muscles are separated and connective tissue is cut to expose the womb.
- 4. Each individual fibroid is removed surgically.
In some cases, the surgeon first injects a drug called Pitressin into the fibroid to stop its blood supply for 20 mins in order to reduce bleeding when removing the fibroids. Or a tourniquet is used for the same purpose. - 5. After removal of the fibroids, each layer of tissue in the womb is carefully stitched together.
- 6. All incisions are closed up with either stitches or staples.
The whole operation can take several hours to complete, depending on the size and location and number of fibroids to be removed. Keyhole procedure in some cases takes longer than open abdominal surgery.
When the operation is over, the anaesthetist will bring you back to consciousness. You will then be moved to the recovery room where you are being watched by the anaesthetist and given oxygen. You will continue to wake up, feel drowsy and weak for a little while. Specially trained nurses will care for you in the recovery room until you are fine to move to the ward.
What happens AFTER surgery?
When you wake up from the operation, you will notice that you have the following:
- An oxygen mask to help you breathe.
- A drip in the arm to give fluids, blood, plasma.
- A temporally bladder catheter.
- A drain from the wound if you have open surgery.
- A pain relieve pump:
Either a PCA (patient controlled analgesia). You have a handheld device where you can press every time you want to give yourself a dose of the pain killer.
Or an epidural pump which delivers the pain killer via your back.
Generally,
- You will feel extremely tired and sleepy.
- If you have a keyhole (laparoscopic) myomectomy, it is likely that you feel some shoulder-tip pain and/or abdominal bloating or pain due to the carbon dioxide gas used in the operation.
- For the next few days, you may be given anticoagulant injection to prevent DVT such as Clexane.
- The PCA for pain relief will be discontinued within 48 hours and you will be given oral pain killers (paracetamol, diclofenac, dihydrocodeine or morphine).
- Tell your nurses as soon as you pass wind or a bowel motion because this shows that your digestive system is getting back to normal. If you do not open your bowel after 3 days, you will be given suppositories to help.
- The urinary catheter will be removed once you are able to make yourself to the toilet.
- You will have 1-2 wound drain bottles to prevent blood from collecting in the wound and causing an infection. This is usually disconnected within 2 -3 days.
What are the self-care tips while I am in the hospital?
Your self-care guide involves performing activities that aid your recovery.
Self-care Tips for you while in hospital include:
| Time post-operation | What to do |
| First day post-op | Start drinking small sips of water to kick starts your gut into working. |
| Sit up right, especially out of bed. This helps to prevent chest infection. | |
| Start moving round. Wear your TED socks to help to prevent DVT. | |
| From second day to discharge time (5 to 6 days) | Try to move around more and become independent. Drink plenty of fluid & walk around to help your bowel working again. |
| Do pelvic floor exercise per instructions from the physiotherapist. | |
| If you need to cough you can hold your stomach, as this will give extra support. |
Going home....
Depending on your speed of recovery, you are going hone within 3 to 7 days after open abdominal surgery and in a day or two after keyhole procedure. You will normally be given an appointment to be seen in the outpatients? clinic in 3 months? time.
Care At Home Guide
- The pinkish/brown vaginal discharge continues for 10-14 days post-op. This is normal as part of the healing process.
- Carry on with pelvic floor exercise per instructions from the physiotherapist.
- Most importantly, keep the wound (incision site) clean and dry. There is no need to put any dressing over it. Apply daily dry antiseptic spray such as Savlon Dry Antiseptic or Betadine Dry Spray (you can buy from pharmacy). The key objective here is to avoid infection for healing to take place.
- A DO and DON'T Table is compiled for you as a self-care at home guide, as always, use your common sense as well.
| Time post-op | DO | DON'T |
| Week 1 to 2 | (a) Use sanitary towels instead of tampons. (b) When you have a bath or shower, use only unscented bath/shower gel or soap around the wound area. Pat dry your wound afterwards. (c) Avoid vaginal lubricant, gel or cream. (d) Start gentle walking around the house in week 1. |
(a) DON'T lift anything heavier than a full kettle. (b) DON'T drive. (c) DON'T have sexual intercourse. |
| Week 3 to 5 | (a) Gently increase your physical activities. (b) Allow rest time throughout the day. (c) Start short walk in week 2. |
(a) DON'T put anything inside your vagina. (b) DON'T drive. (c) DON'T have sexual intercourse. |
| Week 6 Onwards | (a) Resume light work. (b) If you have no pain and you are confident to handle the car, you can start driving. If in doubt, see your GP. (c) You can start sexual intercourse if you have no pain or vaginal bleeding. If you experience pain or bleeding after sex, contact your GP for advice. (d) Return to heavier work and all activities without restrictions in week 10. |
What symptoms to call for emergency medical attention?
While it is unusual to have problem once you are at home, seek immediate medical attention by contacting your Gynaecology Emergency Unit if any of the following symptoms occurs:
(a) Fever with temperature above 38 degree C.
(b) Nausea and vomiting.
(c) Severe and increasing pain.
(d) Increased red blood/clots bleeding from the vagina.
(e) Foul-smelling vaginal discharge (yellow/green colour).
(f) Discharge from wound or wound opening.
(g) Burning pain when passing urine.
(h) Difficulty or unable to pass urine.
(i) Sudden chest pain or shortness of breath.
(j) Pain, swelling or redness in the calf.
Source: Figure 1A and 2 are from Laparascopic Hysterectomy by Francesco Fanfani et al. (2012) CIC Edizioni Internazionali.
Last updated on Monday 1 February 2021 11:57 am.
Related Topics
Jargon Buster
Fibroids FAQs
Adhesion & Asherman's Syndrome
Fibroids & Intertility
Fibroids & Cancer
Operation Clips

Courtesy of Dr Rajesh Varma